

Vous êtes ici : UFR Simone Veil - santéFRFormation continueSeptic shock01. Detecting hypovolaemia
- Publié le 3 février 2023
- Version PDF
01. Detecting hypovolaemia
This is the first step of the examination, given the modifications that hypovolemia can induce, notably in the parameters of systolic function of the left ventricle. We have demonstrated the reliability of the collapsibility index of the superior vena cava (SVC) in patients on assisted ventilation in deciding on blood volume expansion. For this a longitudinal view of the SVC must be recorded, by coupling motion mode (TM-mode) with two-dimensional mode so as to study SVC size variations during a respiratory cycle.
The collapsibility index is calculated as maximum diameter - minimum diameter / maximum diameter.
The SVC is subject to intra-thoracic pressure, and increase in this pressure on insufflation can, in the case of hypovolemia, result in a large diameter decrease or even collapse of the SVC.
Longitudinal view of the superior vena cava by transesophageal route, in 2D mode coupled to M-mode, in a patient on assisted ventilation presenting no respiratory variation in the diameter of the superior vena cava.
Same view in a patient with partial inspiratory collapse of the superior vena cava, suggesting hypovolemia and the need for blood volume expansion.
A collapsibility index above 36% indicates the need for vascular filling which, if sufficient, will lead to significant increase in cardiac flow and decrease in SVC diameter variations during insufflation.
Patient on assisted ventilation for septic shock of pulmonary origin. The longitudinal view shows complete inspiratory collapse of the superior vena cava. Note that the patient presents complete arrhythmia caused by atrial fibrillation.
In the absence of an esophageal probe, or for an overview, echocardiography by the subxiphoid route can be done. It visualizes the inferior vena cava (IVC) and can be used to calculate the distensibility index, to decide whether or not to perform blood volume expansion. The distensibility index of the IVC is calculated as maximum diameter - minimum diameter / minimum diameter.
Unlike the SVC, the IVC is not subject to intra-thoracic pressure, and so tends to increase in size at each insufflation, especially if hypovolemia is present.
This index is, however, less reliable than the collapsibility index of the SVC as it depends, among other things, on intra-abdominal pressure, which is the external pressure on the IVC. In certain conditions of high abdominal pressure, variations in IVC diameter can thus be attenuated.
Media

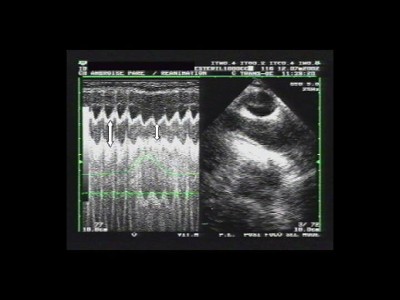


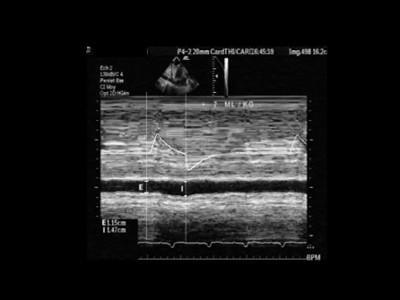

Figure 1 : the pressure signal in the airways appears in green on the screen.
Maximal and minimal diameters are indicated by the arrows.
Figure 2 : E: Expiration, I: Inspiration
Significant increase of IVC diameter related to tidal volume in a septic patient