

Vous êtes ici : UFR Simone Veil - santéFRFormation continueCardiac tamponade02. Hemodynamic aspects
- Publié le 9 février 2023
- Version PDF
02. Hemodynamic aspects
Cardiac output plummets during CT, and heart rate accelerates. The arteriovenous difference increases. This precarious hemodynamic situation is accompanied by metabolic acidosis.
Systemicarterial pressure is low and this drop in pressure is particularly marked on inspiration. Monitoring of arterial pressure reveals an inspiratory reduction in systemic pulse (1,2), which may even be abolished (pulsus paradoxus).
Pulmonaryartery pressure also is subject to large respiratory variations which are almost completely out of phase with the systemic variations. The pulmonary pulse is amplified by inspiration and diminished by expiration (Figure 8, Figure 9) (2).
Left atrial pressure, determined by measurement of the pulmonary artery occlusion pressure, is abnormally high (3) with a mean value close to the pericardial pressure. Transmural pressure is therefore very low but varies with respiration: nil on inspiration but slightly positive on expiration(4,5).
Centralvenous pressure is abnormally high with a mean value identical to that of the pericardial pressure (equalization of pressures). The transmural right atrial pressure is therefore permanently close to zero. It undergoes few respiratory variations. Transmural pressure is slightly positive on systole and nil during diastole (4,6).
The dimensions of the cardiac chambers are reduced. This reduction in size affects the left chambers (7) but is more marked in the right atrium, which may even collapse on diastole (Fig. 2), and at the right ventricle, where collapse is also sometimes seen (Figure 4, Figure 12) (8-11).
Film 2 : Right atrial collapse in diastole during cardiac tamponade, observed by the subcostal route EP: pericardial effusion; OD: right atrium The respiratoryseptal movement is abnormally accentuated, because of flattening and a shift towards the left ventricular chamber on inspiration, and bulging towards the right ventricular chamber on expiration (12).
Film 4 : Apical four-chamber view showing the right (RV) and left (LV) ventricles. In this patient with cardiac tamponade, inspiration is responsible for improved filling of the right ventricle and restriction of the left ventricle, visualized by movement of the interventricular septum towards the left ventricle. The opposite phenomenon is seen on expiration.
Film 5 : In the same patient as in film 4, the small-axis view of the left ventricle shows the same phenomenon. RV: right ventricle, LV: left ventricle.
The aortic and pulmonary flow velocities studied by Doppler echocardiography have an appearance highly superimposable on that of the pulses. The inspiration is accompanied by a reduction in aortic flow velocity which is restored on expiration, whereas the reverse is true for the pulmonary flow velocity (13).
Film 6 : Pulsed Doppler in the pulmonary artery enabling quantification of the systolic ejection volume of the right ventricle. Note the cyclic nature of this ejection: the ejection volume increases at each inspiration, and decreases on each expiration.
The mitral and tricuspidflow velocities have a particular Doppler appearance, with reduction of the normally predominant E-wave and preponderance of the A-wave, which is normally secondary. Furthermore, the respiratory variation of these flow velocities is abnormally marked, with accentuated reduction of the mitral flow on inspiration and accentuated reduction of the tricuspid flow on expiration (4,13).
Inferior caval flow studied by Doppler, where necessary using the subhepatic veins whose axis is more favorable, always comprises an anterograde systolic flow. But the anterograde diastolic flow is abolished and replaced by a reflux (6).
Film 7 : Pulsed Doppler in the subhepatic vein, via the subcostal route, allowing study of the characteristics of right atrial filling. On expiration, note the absence of diastolic filling (adiastole) and the presence of reverse flow, filling being exclusively systolic. On inspiration, filling increases and diastolic flow reappears.
Systemicarterial pressure is low and this drop in pressure is particularly marked on inspiration. Monitoring of arterial pressure reveals an inspiratory reduction in systemic pulse (1,2), which may even be abolished (pulsus paradoxus).
Pulmonaryartery pressure also is subject to large respiratory variations which are almost completely out of phase with the systemic variations. The pulmonary pulse is amplified by inspiration and diminished by expiration (Figure 8, Figure 9) (2).
Left atrial pressure, determined by measurement of the pulmonary artery occlusion pressure, is abnormally high (3) with a mean value close to the pericardial pressure. Transmural pressure is therefore very low but varies with respiration: nil on inspiration but slightly positive on expiration(4,5).
Centralvenous pressure is abnormally high with a mean value identical to that of the pericardial pressure (equalization of pressures). The transmural right atrial pressure is therefore permanently close to zero. It undergoes few respiratory variations. Transmural pressure is slightly positive on systole and nil during diastole (4,6).
The dimensions of the cardiac chambers are reduced. This reduction in size affects the left chambers (7) but is more marked in the right atrium, which may even collapse on diastole (Fig. 2), and at the right ventricle, where collapse is also sometimes seen (Figure 4, Figure 12) (8-11).
Film 2 : Right atrial collapse in diastole during cardiac tamponade, observed by the subcostal route EP: pericardial effusion; OD: right atrium The respiratoryseptal movement is abnormally accentuated, because of flattening and a shift towards the left ventricular chamber on inspiration, and bulging towards the right ventricular chamber on expiration (12).
Film 4 : Apical four-chamber view showing the right (RV) and left (LV) ventricles. In this patient with cardiac tamponade, inspiration is responsible for improved filling of the right ventricle and restriction of the left ventricle, visualized by movement of the interventricular septum towards the left ventricle. The opposite phenomenon is seen on expiration.
Film 5 : In the same patient as in film 4, the small-axis view of the left ventricle shows the same phenomenon. RV: right ventricle, LV: left ventricle.
The aortic and pulmonary flow velocities studied by Doppler echocardiography have an appearance highly superimposable on that of the pulses. The inspiration is accompanied by a reduction in aortic flow velocity which is restored on expiration, whereas the reverse is true for the pulmonary flow velocity (13).
Film 6 : Pulsed Doppler in the pulmonary artery enabling quantification of the systolic ejection volume of the right ventricle. Note the cyclic nature of this ejection: the ejection volume increases at each inspiration, and decreases on each expiration.
The mitral and tricuspidflow velocities have a particular Doppler appearance, with reduction of the normally predominant E-wave and preponderance of the A-wave, which is normally secondary. Furthermore, the respiratory variation of these flow velocities is abnormally marked, with accentuated reduction of the mitral flow on inspiration and accentuated reduction of the tricuspid flow on expiration (4,13).
Inferior caval flow studied by Doppler, where necessary using the subhepatic veins whose axis is more favorable, always comprises an anterograde systolic flow. But the anterograde diastolic flow is abolished and replaced by a reflux (6).
Film 7 : Pulsed Doppler in the subhepatic vein, via the subcostal route, allowing study of the characteristics of right atrial filling. On expiration, note the absence of diastolic filling (adiastole) and the presence of reverse flow, filling being exclusively systolic. On inspiration, filling increases and diastolic flow reappears.
Media
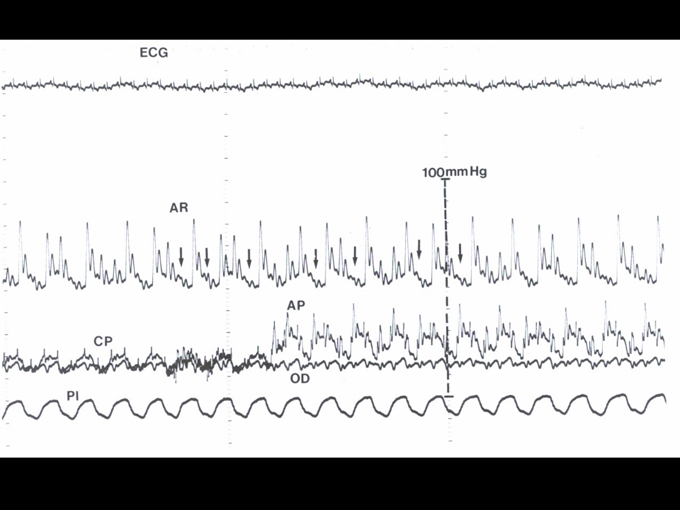
Figure 8 : In a patient presenting a clinical picture of cardiac tamponade, simultaneous recording of an electrocardiogram (ECG), radial artery pressure (AR), pulmonary artery pressure (AP), pulmonary capillary pressure (or pulmonary artery occlusion pressure, CP), right atrial pressure (OD), and esophageal pressure (Pl), which reflects pleural pressure (Pl). On inspiration, marked by a drop in pleural pressure, radial pressure decreases, possibly leading even to complete disappearance of the pulse (arrows). With the pulmonary pulse note also the phase contrast, which is accentuated on inspiration. Lastly, note the equalization of the right (OD) and left (CP) filling pressures in the inspiratory phase, and the restoration of a physiological gradient (CP>OD) in the expiratory phase.
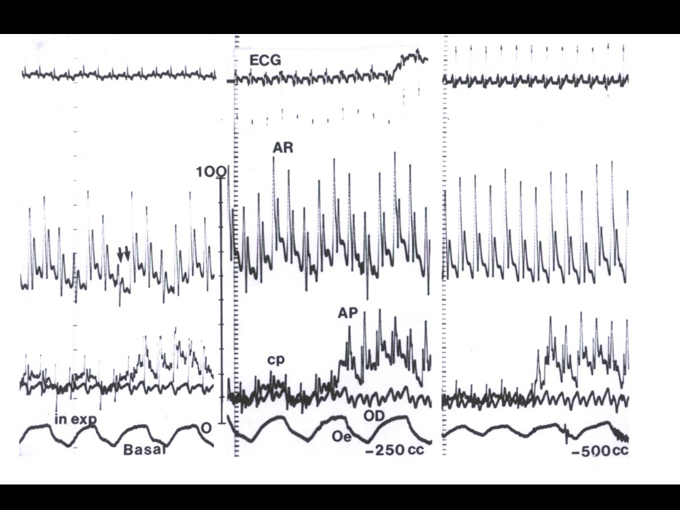
Figure 9 : In a patient presenting a clinical picture of cardiac tamponade, three successive recordings of the electrocardiogram (ECG), radial artery pressure (AR), pulmonary artery pressure (AP), pulmonary capillary pressure (or pulmonary artery occlusion pressure, CP), right atrial pressure (OD), and esophageal pressure (Oe), which reflects pleural pressure (in: inspiration, exp: expiration). These three recordings were made during progressive removal of fluid effusion by pericardial puncture: left, baseline recording before fluid removal; middle, recording after removal of 250 cc; right, recording after removal of 500 cc. Note the progressive restoration of a correct radial artery pressure, with reappearance of a pulse in the inspiratory phase. Note too the phase contrast between the systemic pulse and the pulmonary pulse.
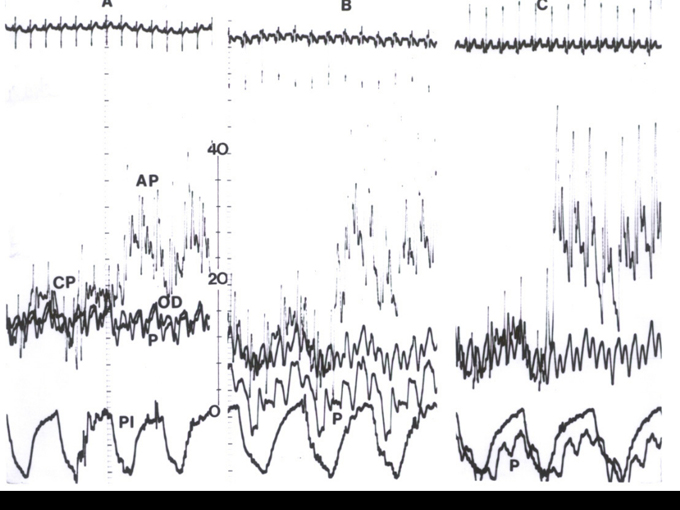
Figure 10 : In a patient presenting a clinical picture of cardiac tamponade, three successive recordings of the electrocardiogram (ECG), pulmonary artery pressure (AP), pulmonary capillary pressure (or pulmonary artery occlusion pressure, CP), right atrial pressure (OD), pericardial pressure obtained on puncture (P), and pleural pressure (Pl), obtained on simultaneous removal of pleural effusion. These three recordings were made during progressive removal of the fluid effusion by pericardial puncture: left, baseline recording before removal; middle, recording after removal of 250 cc; right, recording after removal of 500 cc. Note the high (17 mmHg) right atrial pressure (or central venous pressure) which is equal to the pericardial pressure, on the left of the recording. The removal of the pericardial effusion results in a drop in right atrial pressure, accompanied by a much more marked decrease in pericardial pressure, which finally becomes equal to the pleural pressure at the end of fluid removal. The transmural central venous pressure, which was initially nil, therefore becomes positive.
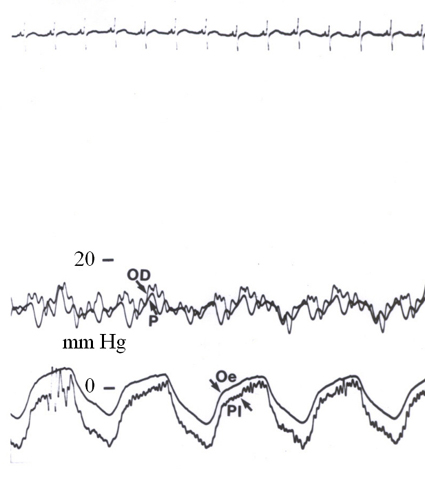
Figure 11 : In a patient presenting a clinical picture of cardiac tamponade, simultaneous recording of the electrocardiogram (ECG), right atrial pressure (OD), pericardial pressure (P), esophageal pressure (Oe), and pleural pressure (Pl). Note the virtual equalization of the pericardial and right atrial pressures, although the latter is slightly higher on ventricular systole (between the R-wave peak and the T-wave of the ECG). The recording can also be used to check that measurement of esophageal pressure gives a good indication of pleural pressure.
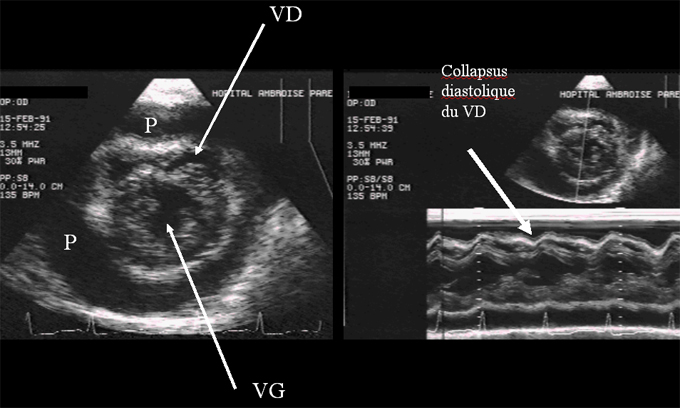
Figure 12 : Short-axis examination of the right (VD) and left (VG) ventricles in a patient presenting pericardial effusion (P). The diastolic collapse of the RV is visible both on the two-dimensional view (left) and in M-mode (right).
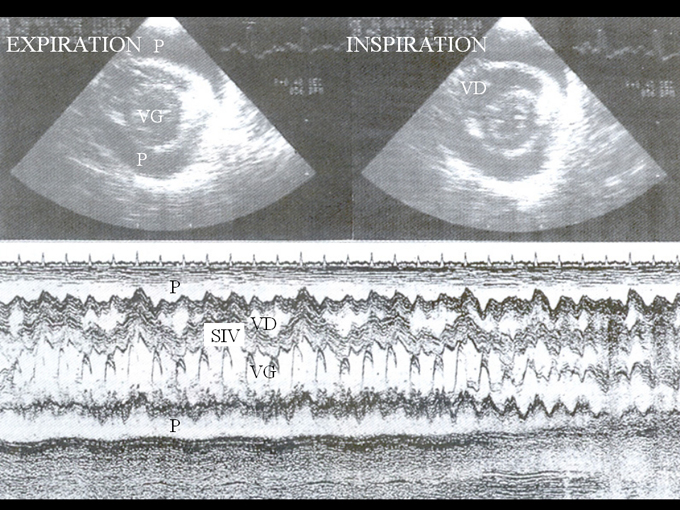
Figure 13 : Short-axis examination of the right (VD) and left (VG) ventricles in a patient presenting pericardial effusion (P). The two-dimensional examination (top) reveals septal shift, increase in RV size, and reduction in LV size, which occur on inspiration (right), compared to expiration (left).These respiratory variations are particularly well demonstrated by M-mode examination (bottom) which shows the cyclic respiratory shift of the interventricular septum (IVS).
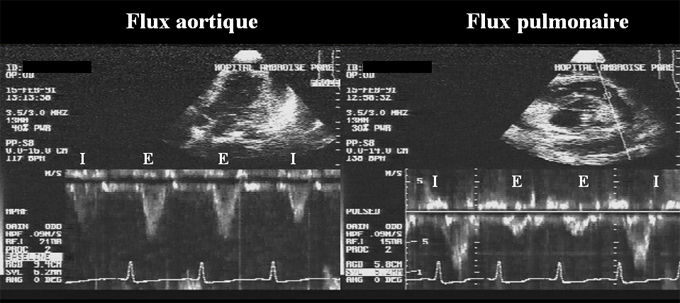
Figure 14 : Recording of aorta (left) and pulmonary artery (right) Doppler flow in a patient presenting cardiac tamponade. Note the phase contrast of these flows with an inspiratory decrease in aorta flow and an expiratory reduction in pulmonary flow. This phase contrast is the same as that seen on the invasive recording of systemic and pulmonary pulses presented in Fig. 8 and Fig. 9.
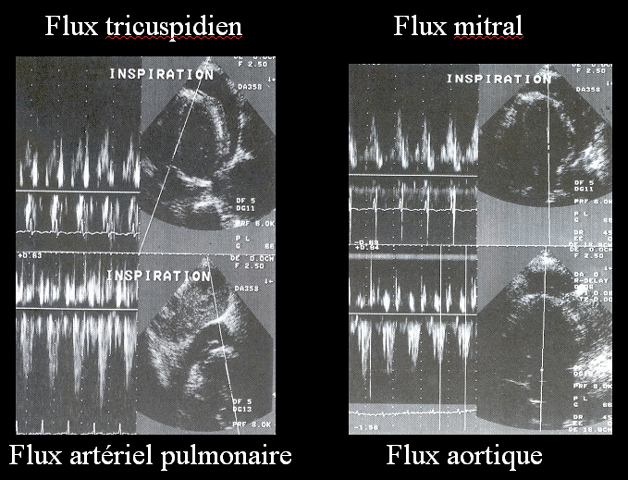
Figure 15 : Appearance of the four valve flows detected by Doppler in a patient in sinus rhythmpresenting cardiac tamponade. Note the inspiratory increase in right flows (tricuspid and pulmonary) and the inspiratory decrease in left flows (mitral and aortic).
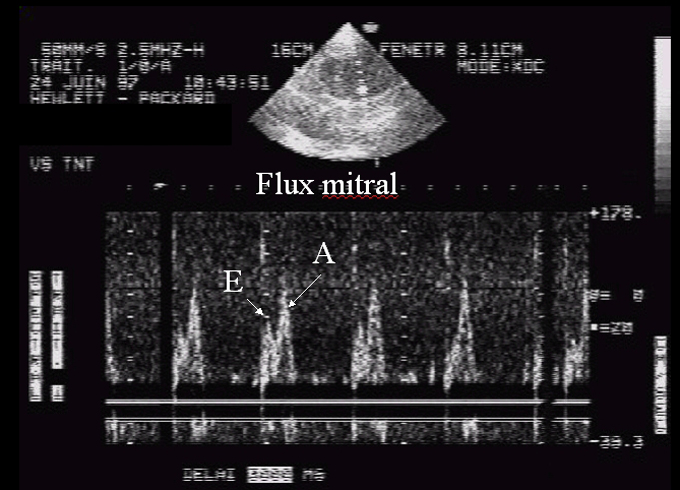
Figure 16 : Appearance of mitral Doppler flow in a patient in sinus rhythmpresenting cardiac tamponade, illustrating deficient left ventricular relaxation. The E-wave (rapid filling) is reduced, while the A-wave induced by atrial systole is predominant. An identical appearance of deficient right ventricular relaxation is observed at the tricuspid valve, as illustrated in Fig. 16.
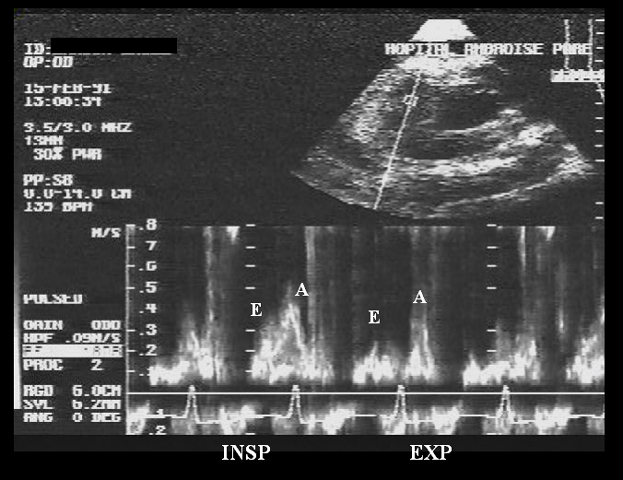
Figure 17 : Appearance of the tricuspid Doppler flow in a patient in sinus rhythmpresenting cardiac tamponade, illustrating deficient right ventricular relaxation. The E-wave (rapid filling) is reduced, while the A-wave induced by atrial systole is predominant. Note the respiratory variations in anterograde tricuspid flow, which are responsible for right ventricular diastolic filling. The flow is greatly reduced during expiration (EXP) and is restored during inspiration (INSP).
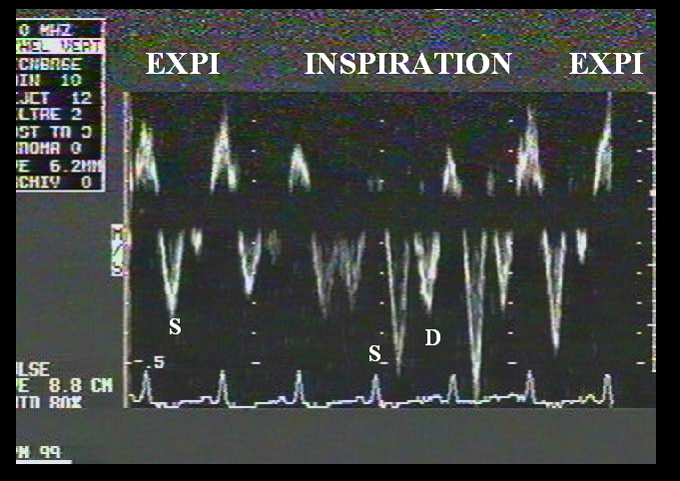
Figure 18 : Appearance of inferior vena caval flow, recorded by Doppler echocardiography of the subhepatic vein. Note the inspiratory accentuation of the systolic wave (S), the expiratory disappearance of the diastolic wave (D), which reappears on inspiration, and the occurrence of a significant retrograde wave (directed upwards) on expiration.
Contents
00. Cardiac tamponade
01. Pathophysiological aspects
01.1 Atrioventricular competition
01.2 Ventricular-ventricular competition
01.3 Impact of respiratory variations
01.4 Ventricular interaction
01.5 Mechanical intervention of the pulmonary vessels ("pooling")
02. Hemodynamic aspects
03. Treatment
04. References
01. Pathophysiological aspects
01.1 Atrioventricular competition
01.2 Ventricular-ventricular competition
01.3 Impact of respiratory variations
01.4 Ventricular interaction
01.5 Mechanical intervention of the pulmonary vessels ("pooling")
02. Hemodynamic aspects
03. Treatment
04. References