

Vous êtes ici : UFR Simone Veil - santéFRFormation continueAcute Cor Pulmonale06. Acute Cor Pulmonale complicating massive pulmonary embolism
- Publié le 9 février 2023
- Version PDF
06. Acute Cor Pulmonale complicating massive pulmonary embolism
The most frequent cause of acute cor pulmonale is obstruction of at least two lobar arteries by massive PE. Kasper was the first to underscore the value of echocardiography when assessing a patient suspected to have PE (12). He quantified right ventricular dilatation using the ratio of the ventricular diameters in M-mode. In view of the deformation of the right ventricle when it dilates, the area ratio we have proposed (1) is more reliable: a simple ratio of diameters ignores apical deformation.
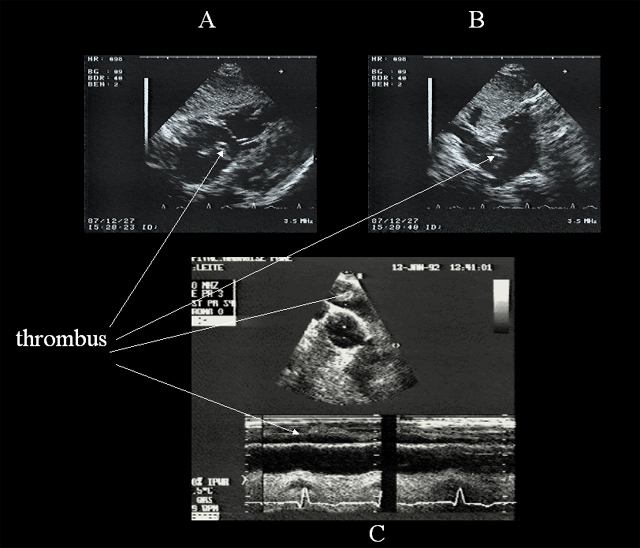
Using our echocardiographic definition of ACP, which combines right ventricular dilatation and paradoxical septal motion, we noted ACP in 61% of 161 successive patients presenting massive PE. Diagnosis is usually made by TTE, since assisted ventilation is rarely used in a patient presenting massive PE. However, in certain emergency patients on assisted ventilation because of cardiorespiratory arrest, TEE can give an immediate diagnosis by detecting ACP, and even by visualizing the thrombus (13).
A thrombus in the right chamber is rarely visualized by TTE.
Acute Cor Pulmonale during PE indicates a major obstruction but is not always accompanied by circulatory insufficiency, as defined by the need to use vasoactive drugs to maintain systolic blood pressure above 90 mmHg (10). Circulatory insufficiency is, however, frequent: we observed it in two thirds of patients with ACP complicating PE (10). When the patient does not develop metabolic acidosis, the prognosis of this circulatory insufficiency is excellent, with vasoactive support for a few hours using dobutamine in first-line treatment (14), and then adrenaline or norepinephrine if dobutamine does not rapidly maintain the blood pressure. Metabolic acidosis marked by a base deficit above 5 mmol/l is a serious sign, and the only sign in our opinion that justifies use of thrombolytic agents (10).
Media
Contents
01. Reminder: ventricular independance
02. Principal echocardiographic views used to study detect ACP
03. Systolic overload
04. Diastolic overload
05. Effects of acute cor pulmonale on the left ventricle
06. Acute Cor Pulmonale complicating massive pulmonary embolism
07. Acute Cor Pulmonale complicating acute respiratory distress syndrome
08. Acute Cor Pulmonale in other clinical settings
09. References